Case Presentation
A 62-year-old retired teacher presented with progressive back pain and bilateral leg pain, significantly affecting her ability to walk and perform daily activities. Symptoms had been worsening over 2 years despite conservative treatments.
Initial Assessment
- Patient: 62-year-old female, retired teacher
- Chief Complaint: Chronic back pain with bilateral leg pain
- Duration: 2 years of progressive symptoms
- Functional Impact: Limited walking distance (<100 meters)
- Previous Treatment: Physical therapy, medications, epidural injections
Diagnostic Evaluation
Clinical Examination
Physical Findings:
- Gait: Antalgic gait with limited walking distance
- Motor Strength: Grade 4/5 in both lower extremities
- Sensation: Decreased sensation in L4-L5 dermatomes bilaterally
- Reflexes: Diminished patellar and Achilles reflexes
- Special Tests: Positive slump test bilaterally
Imaging Studies
X-ray Lumbar Spine:
- Degenerative Changes: Grade 2 spondylolisthesis at L4-L5
- Disc Height: Reduced disc height at multiple levels
- Facet Arthropathy: Severe facet joint degeneration
- Instability: Dynamic instability on flexion-extension views
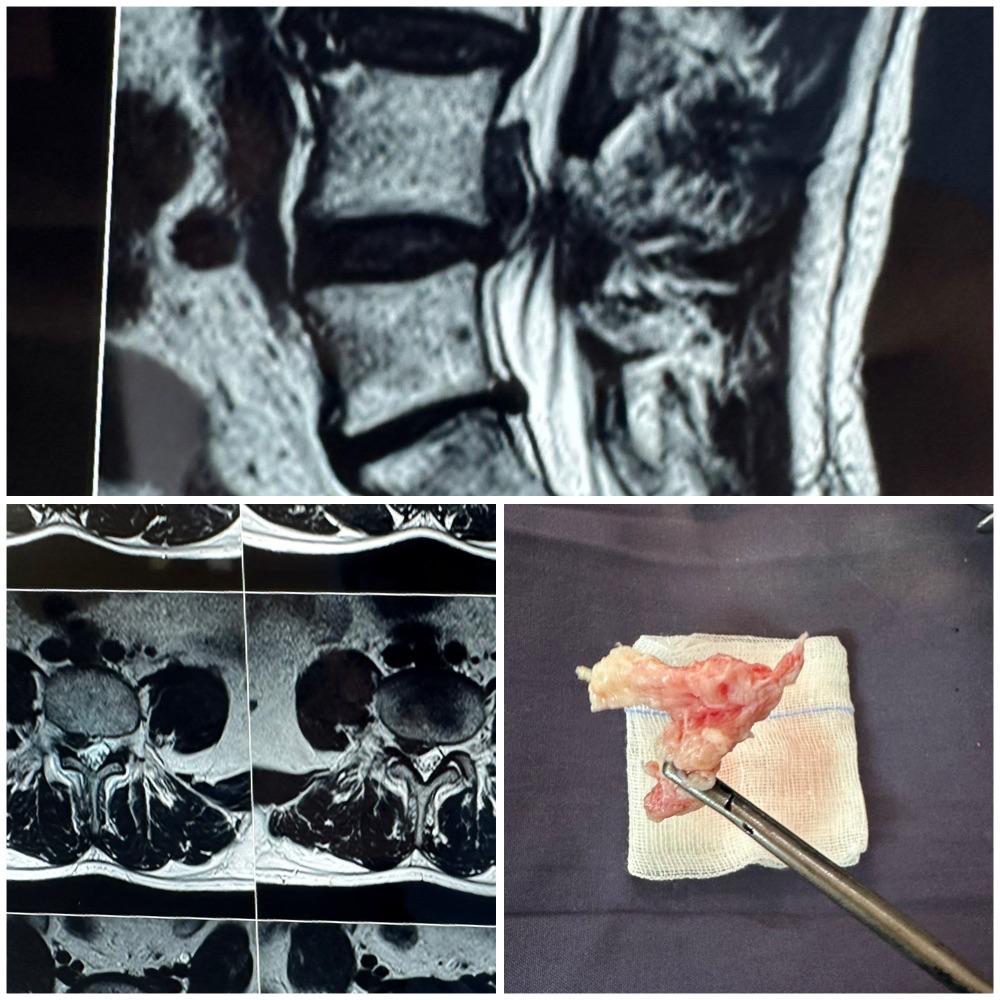
MRI Lumbar Spine:
- Spinal Stenosis: Severe central canal stenosis at L4-L5
- Foraminal Stenosis: Bilateral foraminal narrowing
- Disc Herniation: Multiple disc bulges
- Nerve Compression: Significant nerve root compression
Treatment Planning
Indications for Surgery
Surgical intervention was recommended due to:
- Progressive Neurological Deficit: Motor weakness
- Severe Pain: Uncontrolled with conservative measures
- Functional Limitation: Inability to walk reasonable distances
- Imaging Correlation: Significant compression matching symptoms
Surgical Plan
Procedure Recommended:
- L4-L5 Decompression: Laminectomy and foraminotomy
- Spinal Fusion: Posterior lumbar interbody fusion (PLIF)
- Instrumentation: Pedicle screw fixation
- Bone Graft: Autograft with allograft augmentation
Surgical Procedure
Pre-operative Preparation
- Medical Optimization: Cardiac clearance, anemia correction
- Anesthesia: General anesthesia with invasive monitoring
- Positioning: Prone position on spinal table with padding
- Equipment: Spinal instrumentation set, microscope, neuromonitoring
Surgical Technique
Approach and Exposure:
- Incision: Midline incision from L3 to S1
- Dissection: Subperiosteal dissection of paraspinal muscles
- Instrumentation: Pedicle screw placement at L4 and L5
- Verification: Fluoroscopic confirmation of screw placement
Decompression:
- Laminectomy: Complete removal of L4 lamina
- Foraminotomy: Bilateral foraminotomy at L4-L5
- Facetectomy: Partial facetectomy for adequate decompression
- Ligamentum Flavum: Removal of thickened ligamentum flavum
- Disc Removal: Discectomy at L4-L5 level
Fusion and Reconstruction:
- Disc Space Preparation: Endplate preparation and distraction
- Cage Placement: Interbody cage with bone graft
- Compression: Segmental compression for stability
- Rod Placement: Contoured rods connecting pedicle screws
- Final Compression: Locking screws in compression
Intra-operative Monitoring
- EMG Monitoring: Continuous nerve monitoring
- SSEP: Somatosensory evoked potentials
- MEP: Motor evoked potentials
- Wake-up Test: No neurological changes detected
Post-operative Care
Immediate Post-operative Period
- ICU Care: 24-hour monitoring in ICU
- Pain Management: Epidural analgesia and PCA pump
- Mobilization: Ambulation on postoperative day 2
- Hospital Stay: 5 days for monitoring and rehabilitation
Rehabilitation Protocol
Week 1-2:
- Bed rest with bathroom privileges
- Gentle range of motion exercises
- Deep breathing and incentive spirometry
- Wound care and monitoring
Week 3-6:
- Progressive ambulation with walker
- Core strengthening exercises
- Back extension exercises
- Transition to cane for support
Week 6-12:
- Advanced strengthening program
- Gait training and balance exercises
- Activities of daily living training
- Preparation for return to light activities
Month 3-6:
- Return to normal activities
- Driving clearance
- Recreational activities as tolerated
- Final functional assessment
Outcome and Results
6-Month Follow-up
Clinical Assessment:
- Pain: Significant reduction in back and leg pain
- Function: Walking distance >1 kilometer
- Motor: Full strength restored (5/5)
- Sensation: Normal sensation in lower extremities
Radiological Assessment:
- Fusion: Solid fusion achieved at L4-L5
- Alignment: Restoration of normal alignment
- Hardware: No signs of loosening or failure
- Decompression: Adequate neural decompression confirmed
Patient-Reported Outcomes
- Pain Score: Reduced from 8/10 to 2/10
- Functional Status: Return to daily activities
- Quality of Life: Significant improvement
- Satisfaction: Very satisfied with surgical outcome
Surgical Considerations
Complex Spine Surgery Challenges
- Patient Age: Increased surgical risks in elderly
- Medical Comorbidities: Management of associated conditions
- Bone Quality: Osteoporosis affecting fixation
- Deformity Correction: Restoration of normal alignment
- Neurological Risk: Protection of neural structures
Technical Pearls
- Meticulous Decompression: Adequate neural element release
- Solid Fixation: Proper pedicle screw placement
- Fusion Technique: Proper preparation and grafting
- Blood Loss Management: Minimizing intraoperative bleeding
- Complication Prevention: Proactive complication avoidance
Complications and Management
Potential Complications
- Dural Tear: Cerebrospinal fluid leak management
- Nerve Injury: Intraoperative nerve monitoring protection
- Hardware Failure: Proper technique and patient selection
- Non-union: Smoking cessation and bone health optimization
- Infection: Prophylactic antibiotics and sterile technique
Prevention Strategies
- Pre-operative Optimization: Medical risk factor management
- Intraoperative Monitoring: Continuous neurological monitoring
- Proper Technique: Meticulous surgical execution
- Postoperative Care: Appropriate rehabilitation and monitoring
Long-term Follow-up
Monitoring Schedule
- 6 weeks: Wound check and initial assessment
- 3 months: Fusion assessment and functional evaluation
- 6 months: Final clinical and radiological assessment
- 1 year: Long-term outcome evaluation
Expected Long-term Results
- Pain Relief: 70-80% success rate for pain reduction
- Function: Improved walking ability and daily function
- Durability: Long-lasting fusion and symptom relief
- Quality of Life: Significant improvement in overall well-being
Patient Selection Criteria
Ideal Candidates
- Significant Symptoms: Pain and functional limitation
- Failed Conservative: Adequate trial of non-surgical treatment
- Corresponding Imaging: Radiological findings match symptoms
- Reasonable Health: Appropriate medical fitness for surgery
- Realistic Expectations: Understanding of recovery process
Contraindications
- Severe Medical Illness: Uncontrolled comorbidities
- Active Infection: Systemic or local infection
- Severe Osteoporosis: Poor bone quality for fixation
- Non-compliance: Inability to follow postoperative instructions
Rehabilitation Philosophy
Principles of Recovery
- Early Mobilization: Prevent complications of bed rest
- Progressive Loading: Gradual increase in activity
- Core Strengthening: Support for spinal fusion
- Patient Education: Understanding of limitations and goals
- Long-term Maintenance: Lifetime spine health practices
This case demonstrates successful management of complex spinal stenosis with spondylolisthesis through decompression and fusion surgery. The outcome highlights the importance of proper patient selection, meticulous surgical technique, and comprehensive rehabilitation for optimal results.
For expert evaluation and treatment of complex spine conditions, contact VPL Ortho and Spine Clinic at +91 9042353157.